Oh dear, about 16 months since I last posted here. Still I hope that featured image above gives a sense of spring arriving! I guess some of those months have been pretty affected by the coronavirus pandemic. There’s a little bit more about how that impacted on me and how I spent a lot of those months high up in the Alps, very protected from cv-19. During this time I have been working very hard and been fairly successful getting papers I like accepted (see publication list and CV)
In the last month I have protected some work time away from Emails, data crunching and paper writing and come back to web things. That has resulted in:
My SAFAQ or Rblog. This is a set of Self-Answered Frequently Answered Questions (hence SAFAQ) and is the best way I have found to present how I use R and allows me to do that in a way that I can’t here in WordPress.
That is quite closely linked with:
The CECPfuns R package. R (r-project.org)is a brilliant, open source, completely free system for statistical computation than runs on pretty much any Linux, on Macs and on Windows. It is partly made up of packages of functions and I have written one that I hope will grow into a useful resource for people wanting to use R for therapy and psychology work but wanting a fairly “newbie friendly” rather than R geeky hand with that. It complements the SAFAQ/Rblog. cecpfuns.psyctc.org is a web site built out of the package documentation and all the geeky details are at github.com/cpsyctc/CECPfuns.
Those are both developing quite fast with the latter getting updates daily, sometimes more often, and the former getting new items more often than once a week. I suspect that now I have announced them here, I may do intermittent posts here that just give an update about one or both of those and they will get to be linked more into pages here. There are two more key developments coming up:
My own shiny server here that will provide online apps for data analysis and providing explanations of analytic tools.
A book “Outcome Measures and Evaluation in Counselling and Psychotherapy” written with my better half, Jo-anne Carlyle, that should be coming out through SAGE in late November (and they have just sent us the first proofs exactly to their schedule so perhaps I should start believing that it will come out then.) That is aimed at demystifying that huge topic area and, we hope, making it easier for practitioners both to understand, and critique, it, and to start doing it. That will lean heavily on SAFAQ pages and the apps on the shiny server.
And now, in radical contrast to the featured/header image, something completely different:
An 8Gb Raspberry Pi 4
That’s sitting on my desk, about the size of a small book. It’s a local version of the system that, I hope, will host the shiny server!
Perhaps this post should be a post, or even an FAQ, in my CORE web site, but then I fear it would be taken too formally so it’s here. However, I’ll put a link to this from the CORE blog: this thinking started with one of a sudden slew of Emails I’ve had coming to me via the CORE site.
I won’t name names or Universities but I will say that it came from the UK. I think it could easily have come from other countries but I have the general experience that many countries still have less of this problem, seem less fearful of asking people about unhappiness or even self-destructiveness than many UK ethics committees seem to be.
The specific problem is the idea that if a research project asks people, particularly young people: teenagers or university students, about distress, and particularly about thoughts of self-harm or suicide, that there’s a terrible risk involved and the project shouldn’t happen. This sometimes takes the form of saying that it would be safer only to ask about “well-being” (or “wellbeing”, I’m not sure any of us know if it needs its hyphen or not).
A twist of this, the one that prompted this post, is the idea that the risk might be OK if the researcher using the measure, offering it to people, is clinically qualified or at least training in a clinical course. That goes with a question I do get asked fairly regularly about the CORE measures: “do you need any particular qualifications to use the measures?” which has always seemed to me to be about the fantasy that if we have the right rules about who can do what, everything will be OK.
This post is not against ethics committees. I have worked on three ethics committees and have a huge respect for them. They’re necessary. One pretty convincing reading of their history is that their current form arose particularly out of horrors perpetrated by researchers, both in the US and the UK, and also in the concentration camps. Certainly the US and UK research horrors did lead to the “Institutional Review Board (IRBs)” in the States and the “Research Ethics Committees (RECs)” in the UK. Those horrors that really were perpetrated by researchers, particularly medical researchers, but not only medical researchers, are terrifying, completely unconscionable. It’s clearly true that researchers, and health care workers, can get messianic: can believe that they have divine powers and infallibility about what’s good and what’s bad. Good ethics committees can be a real corrective to this.
Looking back, I think some of the best work I saw done by those ethics committees, and some of my contributions to those bits of work, were among the best things I’ve been involved with in my clinical and research careers so I hope it’s clear this isn’t just about a reasearcher railing against ethics committees. However, my experience of that work brought home to me how difficult it was to be a good ethics committee and I saw much of the difficulty being the pressure to serve, in the Freudian model, as the superego of systems riven with desires, including delusional aspirations to do good through research. I came to feel that those systems often wanted the ethics committee to solve all ethical problems partly because the wider systems were underendowed with Freud’s ego: the bits of the system that are supposed to look after reality orientation, to do all the constant, everyday, ethics they needed done.
In Freud’s system the superego wasn’t conscience: a well functioning conscience is a crucial part, a conscious part, of his ego. You can’t have safe “reality orientation” without a conscience and, as it’s largely conscious, it’s actually popping out of the top of his tripartite model, out of the unconscious. His model wasn’t about the conscious, it was about trying to think about what can’t be thought about (not by oneself alone, not by our normal methods). It was about the “system unconscious”: that which we can’t face, a whole system of the unreachable which nevertheless, he was arguing, seemed to help understand some of the mad and self-destructive things we all do.
In my recycling of Freud’s structural, tripartite, model, only his id, the urges and desires is unequivocally and completely unconscious, the superego has some conscious manifestations and these do poke into our conscious conscience, and the ego straddles the unconscious (Ucs from here on, to speed things up) and the conscious. (I think I’m remembering Freud, the basics, correctly, it was rather a long time ago for me now!)
I’m not saying that this model of Freud’s is correct. After all, Freud with theories, was rather like Groucho Marx with principles, they both had others if you didn’t like their first one …) What I am arguing, (I know, I do remember, I’ll come back to ethics committees and questionnaires in a bit) is that this theory, in my cartoon simplification of it, may help us understand organisations and societies, even though Freud with that theory was really talking about individuals.
As I understand Freud’s model it was a double model. The was combining his earlier exploration of layers of conscious, subconscious and Ucs with this new model with its id, superego and ego. They were three interacting systems with locations in those layers. With the id, ego and superego Freud was mostly interested in their location in unconscious. Implicitly (mostly, I think) he was saying that the conscious (Cs), could be left to deal with itself.
That makes a lot of sense. After all consciousness is our capacity to look after ourselves by thinking and feeling for, and about, ourselves. To move my metaphors on a century, it’s our debugging capability. Freud’s Ucs, like layers of protection in modern computer operating systems, was hiding layers of our functioning from the debugger: our malware could run down there, safely out of reach of the debugger.
The id, superego, ego model is surely wrong as a single metatheory, as a”one and only” model of the mind. It’s far too simple, far too static, far too crude. Freud did build some two person and three person relatedness into it, but it was still a very late steam age, one person, model and desperately weak on us as interactional, relational, networked, nodes, it was a monadic model really.
However, sometimes it fits! My experience on those committees, and equally over many more years intersecting with such committees, is that they can get driven rather mad by the responsibilities to uphold ethics. They become, like the damaging aspects of Freud’s model of the individual’s superego, harsh, critical, paralysing, sometimes frankly destructive. The more the “primitive”: rampant desire (even for good), anger and fears of premature death and disability gets to be the focus, the more they risk losing reality orientation, losing common sense and the more the thinking becomes rigid. It becomes all about rules and procedures.
The challenge is that ethics committees really are there to help manage rampant desire (even for good), anger and fears of premature death and disability. They were created specifically to regulate those areas. They have an impossible task and it’s salutory to learn that the first legally defined medical/research ethics committees were created in Germany shortly before WWII and theoretically had oversight of the medical “experiments” in the concentration camps. When society loses its conscience and gives in to rigid ideologies (Aryanism for example) and rampant desires (to kill, to purify, to have Lebensraum even) perhaps no structure of laws can cope.
OK, so let’s come back to questionnaires. The particular example was the fear that a student on a non-clinical degree course might use the GP-CORE to explore students’ possible distress in relation to some practical issues that might plausibly not help students with their lives, or, if done differently, might help them. The central logic has plausibility. I have no idea how well or badly the student was articulating her/his research design, I don’t even know what it was. From her/his reaction to one suggestion I made about putting pointers to health and self-care resources at the end of the online form, I suspect that the proposal might not have been perfect. Ha, there’s my superego: no proposal is perfect, I’m not sure any proposal ever can be perfect!
What seemed worrying to me was that the committee had had suggested that, as someone doing a non-clinical training, s/he should leave such work and such questionnaires to others.To me this is hard to understand. S/he willhave fellow students who self-harm, some who have thoughts of ending it all. One of them may well decide to talk to her/him about that after playing squash, after watching a film together.
Sure, none of us find being faced with that, easy: we shouldn’t. Sure, I learned much in a clinical training that helped me continue conversations when such themes emerged. I ended up having a 32 year clinical career in that realm and much I was taught helped (quite a bit didn’t but we’ll leave that for now!) It seems to me that a much more useful, less rule bound, reaction of an ethics committee is to ask the applicant “have you thought through how you will react if this questionnaire reveals that someone is really down?” and then to judge the quality of the answer(s). The GP-CORE has no “risk” items. It was designed that way precisely because the University of Leeds which commissioned it to be used to find out about the mental state of its students, simply didn’t want to know about risk. (That was about twenty years ago and it’s really the same issue as the ethics committee issue.)
One suggestion from the committee to the student was only to use a “well-being” measure. Again, this seems to me to be fear driven, not reality orienting. There is much good in “well-being work”, in positive psychology, and there is a very real danger that problem focus can pathologise and paralyse. However, if we only use positively cued items in questionnaires and get a scale of well-being then we have a “floor effect”: we’re not addressing what’s really, really not well for some people. We specifically designed all the CORE measures to have both problem and well-being items to get coverage of a full range of states. The GP-CORE is tuned not to dig into the self-harm realm but it still has problems, the CORE-OM, as a measure designed to be used where help is being offered to people who are asking for it, digs much more into self-harm.
Many people, many younger people, many students, are desperately miserable; many self-harm; tragically, a few do kill themselves. Yes, clinical trainings help some people provide forms of help with this. However, improving social situations and many other things that are not “clinical” can also make huge differences in Universities. (In the midst of industrial action, I of course can’t resist suggesting that not overworking, not underpaying academics, not turning Universities into minimum wage, temporary contract, degree factories, might help.)
Misery, including student misery, is an issue for all of us, not just for some select cadre thought to be able to deal with it by virtue of a training. So too, ethics is everyone’s responsibility. Perhaps we are institutionalising it into ethics committees, into “research governance” and hence putting the impossible into those systems. We create a production line for ethics alongside the production lines for everything else. Too often perhaps researchers start to think we just have to “get this through ethics” and not really own our responsibility to decide if the work is ethical. Perhaps too many research projects now are the production line through which our governments commission the research they want, probably not the research that will question them. Perhaps that runs with the production line that produces docile researchers. It’s time we thought more about ethics ourselves, and both trusted ourselves and challenged ourselves, and our peers, to engage in discussions about that, to get into collective debugging of what’s wrong. Oops, I nearly mentioned the UK elections … but it was a slip of the keyboard, it’ll get debugged out before Thursday … or perhaps it would if I wrote still needing to be on the right conveyor belts, the right production lines.
Oh, that image at the top: commemoration ‘photos, from family albums I would say, of the “disappeared” and others known to have died at the hands of the military, from Cordoba, Argentina. From our work/holiday trip there this summer. A country trying to own its past and not fantasize.
I too was a medical student in 1975. Would I have been brave? Ethical?
This little saga started over a year ago when I helped at a workshop a psychological therapies department held about how they might improve their use of routine outcome measures. They were using the CORE-OM plus a sensible local measure that added details they wanted and for which they weren’t seeking comparability with other data.
In the lunch break someone told me s/he had CORE-OM data from a piece of work done in another NHS setting (with full research governance approval!) The little team that had put a lot of work into a small pragmatic study felt stymied because the Cronbach alpha for their CORE-OM data was .65 and they were worried that this meant the perhaps the CORE-OM didn’t work well for their often highly disturbed clientèle. They had stopped there but thought of asking me about it.
My reaction was that I shared the concern about self-report measures, not just the CORE-OM, perhaps not having the same psychometrics, not working as well, in severely disturbed client groups as in the less disturbed or non-clinical samples in which they’re usually developed. However, I hadn’t thought that would bring the alpha down that low and wondered if they had forgotten to reverse score the positively cued items.
As everyone’s crazily busy I didn’t hear anything for a long while but then got a message that they had checked and the coding was definitely right, would I have a look at their data in case it really was about the client group as they knew I was interested in how severity, chronicity and type of disturbance may affect clients’ use of measures.
I agreed and received the well anonymised data. About 700 participants had completed all the items and the alpha was .65 (not that I really doubted them, I just like to recheck everything!) So I checked the item score ranges though I hadn’t really thought there was likely to be much by way of data entry errors. There wasn’t: just two out of range items in over 23,000. The one was 11 and the other was 403. Changing them to missing, and hence dropping two participants resulted in an alpha of .93 with a parametric 95% confidence interval from .93 to .94, i.e. absolutely typical for CORE-OM data.
I would never have believed that just 0.008% incorrect items could affect alpha that much, even if one was 403 when the item upper score limit is 4: I was wrong! Well, perhaps it’s not quite that low a percentage. If that 11 was 1 for the one item (item22) and another 1 which should have gone into item 23 then perhaps many of the remaining items for that client were wrong; same for 403 for item 28, after all 1, 4, 0 and 3 are all possible item scores on the CORE-OM. That would take the incorrect entries up to 0.08%. However, if something like failure to hit the carriage return is the explanation then there should have been one or more missing items at the end of the entries for that client and their data would never have made it into the computation of alpha. Perhaps a really badly out of range item at a rate of just 0.008% is enough to bring alpha down this much. Only checking back to the original data will tell. I hope they still have the original data.
OK, but does this merit a blog post (well, I’ve got to start somewhere!) I think there are some points of interest.
it shows just how influential a few out of range scores can be
it shows that alpha can sometimes detect this and hooray for the people involved that they did calculate alpha and sensed that something was so wrong that they couldn’t just go ahead with the analyses they had planned
it does show though that simple range checks on items were a quicker and more certain way of detecting what was at root here
it shows that though I think you should always do all the range and coherence checks on data that you can think of making sense for the data …
… it’s stronger to have duplicate data entry but which of us can afford this?
even if you can do duplicate entry (assuming that the clients complete the measures on paper) you should use a data entry system that as far as possible detects impossible or improbable data at the point of entry
(and if you do have direct entry by clients please make sure it does that entry checking and in a user-friendly way)
but while absurd sums of money are put into healthcare data systems and into funding psychological therapy RCTs, where is the money to fund good data entry, clinician research and practice based evidence?
To finish on a gritty note about data entry, at least twenty years ago, before I discovered S+ and R I mainly used SPSS for statistics and back then, for a while, SPSS had a “data entry module”. It was slow ,which was perhaps why they dropped it but it was brilliant: you could set up range checks and all the coherence checks you wanted (pregnant male: I think not). After that died I tended to enter my data into spreadsheets and until about a year ago I was encouraging colleagues I work with around the world to use Excel (yes, I tried encouraging them to use Libre/OpenOffice but everyone had and knew Excel and often weren’t allowed to install anything else). They or I would write data checking into the spreadsheets to the extent that Excel allows and I wrote data checking code in R (https://www.r-project.org/) to double check that and to catch things we couldn’t in Excel. I still use that for one huge project but it’s a nightmare: updates of Windoze and seem to break backwards compatibility, M$’s way of handling local character sets seems to create problems, its data checking seems to break easily and I find it almost impossible to lock spreadsheets so that people can enter data but not change anything else. I’m sure that there are Excel magicians who can do better but I’m equally sure there are better alternatives. At the moment, with Dr. Clara Paz in Ecuador, we’re using the open source LimeSurvey survey software hosted on the server that hosts all my sites (thanks to Mythic Beasts for excellent open source based hosting). If you have a host who gives you raw access to the operating system LimeSurvey is pretty easy to install (and I think it runs on nasty closed source systems too!) Its user interface isn’t the easiest but so far we’ve been able to do most things we’ve wanted to with a bit of thought and the main thing is that it’s catching data entry errors at entry and proved totally reliable so far.
For my own benefit, and in case it’s useful to anyone else, I’m putting a technical blog post here now which I hope will capture the main steps I’ve taken so far.
Location and URLs
I had the existing static HTML site at https://www.psyctc.org/ and I already had a WordPress installation underneath that (my personal site and blog: https://www.psyctc.org/pelerinage2016/ and Mythic Beasts, the excellent service provider who have been supporting my internet presences for years agreed that having one WordPress instance nested in a URL below another was a recipe for trouble so I opted to have the new WordPress instance at https://www.psyctc.org/psyctc/ . Clearly, that’s a bit clumsy and if you don’t have a reason to do this you can probably simply install WordPress into your URL root.
Over the last five years I’ve had experience with a number of commercial WordPress themes in sites I’ve created and that’s left me rather unimpressed with incompatibilities and poor support so these days I prefer to use WordPress’s own free themes. For this I’ve gone for Twenty Fifteen as it seemed to fit what I needed and, making my life simpler, it’s the one to which I’m also retheming and rejigging my CORE System Trust site.
I’m clear that the first thing anyone should do once they’ve chosen a sensible basic theme is to make a “child theme” so you minimise the risk of losing any customisation you make if the them is updated. For that I used the Child Theme Configurator Pro plugin. That’s a paid for extension of that company’s free plugin which wasn’t expensive and I felt was worth paying for but you can make a child theme by hand or using their free plugin (and there are other plugins to do this: I don’t claim to have done more than some simple searching which led me to this one but so far I like it a lot).
Appearance customisation
I’ve tweaked the footer to remove “Proudly” from “Proudly powered by WordPress” as I’m very happy to acknowledge my huge debt to the WordPress world but “proudly” just isn’t my language: they’re the ones who can be proud of this, I’m just grateful! To hack that you have to edit footer.php which the child theme plugin makes very easy though it would be very easy to do if you have pretty much any other route to that file. It’s a small file and easy to understand and to find “Proudly powered” in it and edit that without knowing anything about PHP.
I used the standard customisation options to use the background colour I’d used on a lot of the old pages and used old gifs as identity icons. In case you wonder what they are: they’re a nod to my proud (yes, “proud”) membership of the Institute of Group Analysis) and I created the gifs so long ago that I haven’t the faintest idea now what tools I used but they would have been done in MS DOS!
I replaced the old index.html root html file of www.psyctc.org with a very short one that redirects to https://www.psyctc.org/psyctc/. If you want that code it’s easy to find or you can right click that link above (in most browsers) and grab my file and edit it to point where you want it to (and not here!) As you can see in my new WordPress home page, I renamed the old index.html file and put a link back to that so that anyone wanting the old site can get it easily.
Plugins
I’m trying not to use more plugins than I need and probably the child theme configurator wasn’t strictly necessary but did help me feel safe and guided through that process and supported other things. I’ve installed Google Fonts PRO to customise typography as I’ve used it on two other sites recently but so far I don’t think I’ve actually changed any fonts so perhaps that should go. I’ve used the free plugin Contact Form Email for all my contact forms over the last five years and it’s worked perfectly as far as I can tell and is upgraded rapidly and has a large user base with good reviews so I felt no reason to change from that though I don’t think the settings interface is particularly user friend or intuitive but once you’ve used it a bit that’s no longer an issue.
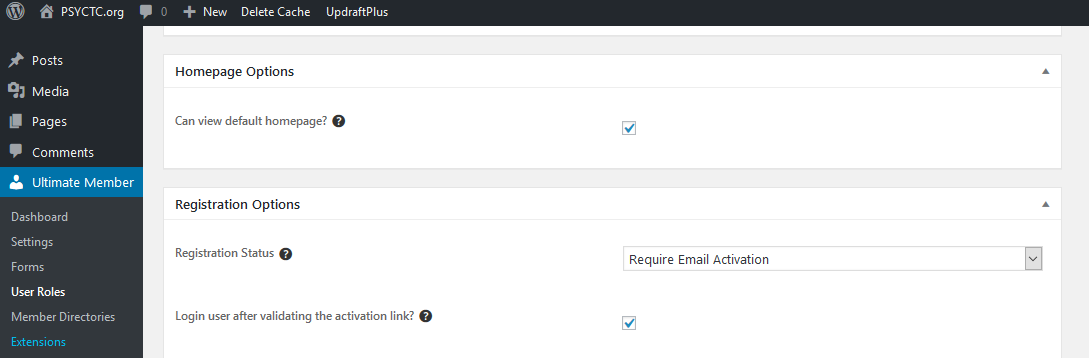
One thing that’s new for me is to require people to subscribe to post comments on this blog and I’ve used the free Ultimate Member plugin to handle that. One thing there that took quite a lot of sleuthing to work out was how you force subscribers to validate their Emails. I think the setting is ridiculously hidden and I had assumed that if you activated the Email template asking people to validate their Email address that requirement would be set automatically. I found the answer eventually at https://wordpress.org/support/topic/registration-confirmation-email-is-not-sent-2/ you set that it in the in the User Roles section of the Ultimate Member menu entries in the WordPress administration panel:
It’s that selection window that has to be switched to “Require Email Activation”.
I’ve installed TinyMCE Advanced and did manage to get it to give me control over font size in pages and posts but it’s clearly not working nicely with the new WordPress “Gutenberg” editor which is a pain. To be brutal, so far I’m pretty unconvinced by the early user experience with Gutenberg but it’s clear that WordPress are committed to it and I think I can see that it will have long term avantages so I’m resisting the temptation to revert to the classical editor. I hope someone, whether it’s Tiny or WordPress or someone else, ends up putting the sort of controls into the default text editor that TinyMCE Advanced did pretty easily for me in the classical editor.
I added the free Relevanssi search plugin. That was actually a mistake when I was trying to work out how to add “search” and eventually I settled for making it accessible from “footer” widget menu in the theme. (I put “footer” in scare quotes as it’s actually not what I consider a footer as located by the theme: this the bottom part of the side menu.) However, Relevanssi looks good so I’ll stick with it.
I have installed the free Google Analytics for WordPress by MonsterInsights plugin (what a name!) and created a Google analytics account for the site. I’d love not to use Google but I do sort of know how to do and use this approach so it stays for now but is on my list to drop if I can.
Security and safety plugins
I’m not sure if Akismet is installed by default in WordPress now or was installed by Mythic Beasts when they did the WP installation for me (I’m getting lazy!) but I have activated it though I’m requiring subscription before posting a comment and using Email subscription validation so it’s going to be a pretty determined real live spammer trying to post comments so perhaps I don’t need it.
As already noted, I’m using the free Ultimate Member plugin to manage subscriptions. The installation had the free Login LockDown plugin installated, again I’m not sure if that comes by default or was added by Mythic Beasts but it looks sensible “by restricting the rate at which failed logins can be re-attempted from a given IP range” which sounds very sensible so that’s staying. I’ve added UpdraftPlus which I use for backups of all my WordPress sites. I use the paid for professional version and their cloud vault: not cheap but feels wise.
Finally, the free WP Super Cache plugin was installed and I’ve had that in all my WP sites and think it really does speed things up (but when you’re making configuration changes and they don’t seem to be working, always switch it off or flush its cache and retry before assuming you’re doing something wrong: I wasted fifteen minutes or so changing the names of the widgets and seeing no change in them before I remembered that one!) I love the company’s map of its employees!
Damn, thought I was finished for now and just remembered that I need to add a privacy statement. Enough here for now!
Rather frighteningly (for me at least) the PSYCTC.org site is at least 23 years old. Its origins were in some pages I created when I worked at St. George’s Hospital Medical School and it’s moved across umpteen hardware platforms since then. Much of it is raw HTML files I created over the years, probably mostly with emacs on Linux systems. That meant it was light and fast when that really mattered as people, including me editing it, might be using dial up modems to get to it. I’m not sure there’s anywhere in the world now where people will be accessing things that way and it’s meant that changing things was not easy. I’ve finally decided to protect a bit of time to shift the site to WordPress which, though it has many faults to my mind, does make maintaining and developing a site easier than coding it in raw HTML! I’ll never have the eye, skills or time to make things look beautiful but at least a minimally modified WordPress theme will look better than anything I can hand craft. I will use this blog space to share technical challenges I hit with the site and generally with using WordPress where I think I found something that might be useful to others, however, it’ll be mainly for thoughts about psychotherapy and counselling research and particularly my fascinations with psychometrics, with what I call “rigorous idiography” and with methodology pretty generally.